



Forecast: The Impact of USAID HIV/AIDS Cuts

by Jared Leibowich
The United States President’s Emergency Plan for AIDS Relief was launched in 2003 to combat HIV/AIDS throughout the world. Probably the most celebrated foreign assistance program of the past 80 years, its primary task is to provide medication to individuals living with HIV. It also works to prevent HIV transmission.
In the first week of Trump’s second term, the administration issued a stop-work order that froze payments and services for foreign aid; subsequently, most foreign aid was suspended. After bipartisan outcry, parts of PEPFAR were granted a waiver to continue “life-saving HIV services,” but there have been major issues with the rollout of the waiver.
In this article, I estimate how many people will die after one year, and through to when Trump’s term ends — if the waiver fails to maintain PEPFAR’s previous life-saving services. I consider several factors in my forecast, which I’ll review to give a window into my estimation process.
How quickly HIV cases are increasing
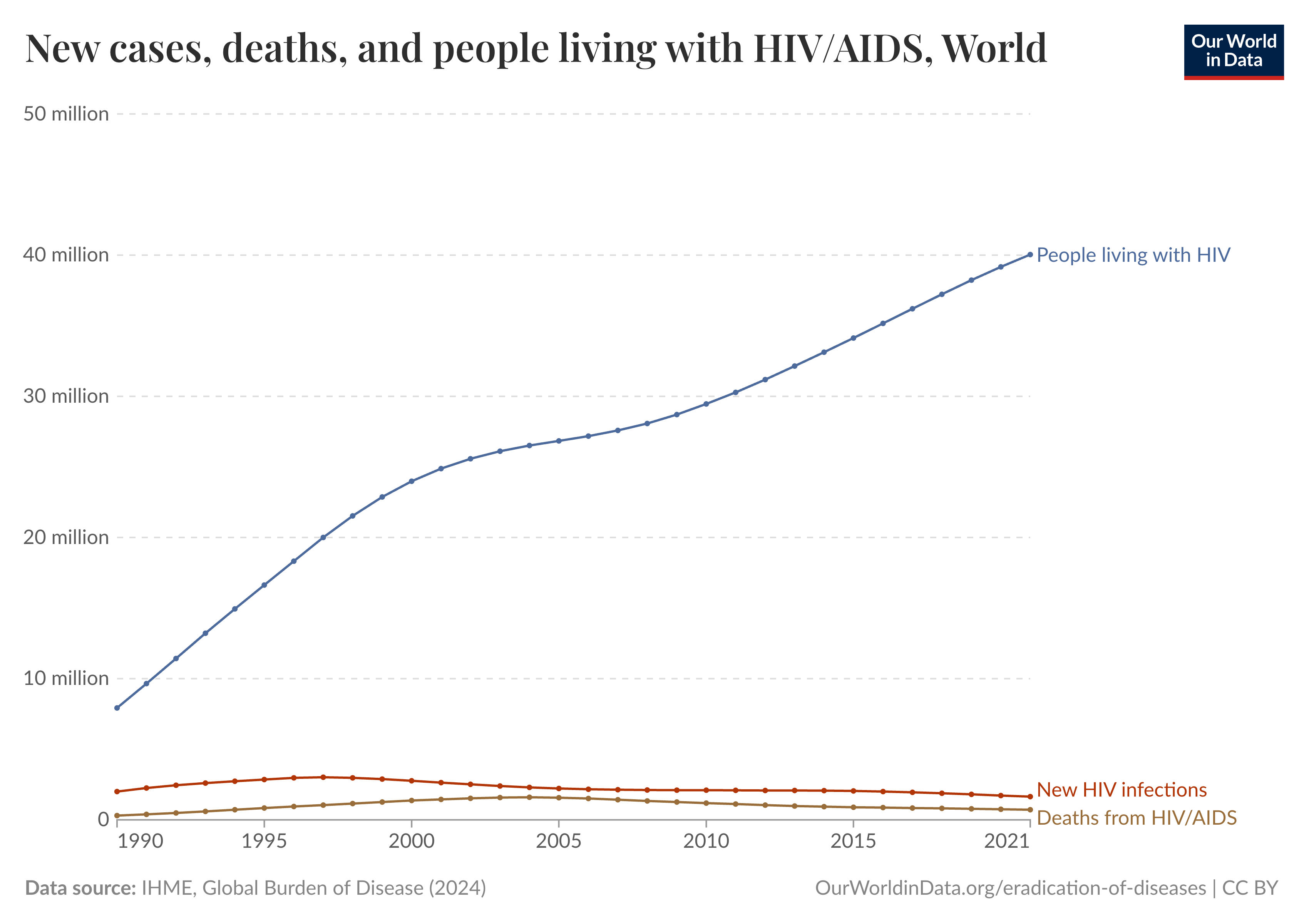
Growth in HIV cases over the past decade has been relatively constant. About one million more people live with the virus each year. In 2021, the last year that Our World in Data documented, about 40 million people lived with HIV. Extending this trend, we can estimate that about 43 million people were living with HIV/AIDS in 2024. The incidence rate is much higher than a million a year, as many people die from AIDS-related deaths: In 2021, the last year for which data is available, that number was 718,000, making the incidence rate around 1.7 million a year.
How many people receive antiretroviral therapy through PEPFAR
Over 20 million people received ART from PEPFAR in 2023, roughly half of the global population living with HIV.
How many cases of HIV are prevented each year because of PEPFAR
The number of new cases of HIV per year has declined from a high of three million in 1997 to 1.65 million in 2021.

The pattern is less predictable here. The rate of decrease actually slowed around the time PEPFAR was launched. One possible explanation is that yearly new cases were on the verge of stabilizing at around 2.25 million, and PEPFAR helped decrease that number. But it is somewhat unexpected that the incidence rate would stabilize between 2008 and 2014 before declining again, given constant support.
Ideally, I could use this information to predict the number of HIV cases prevented each year as a result of PEPFAR, but because I would have very low confidence in the estimates I came up with, I won’t use this number.
How PEPFAR decreases HIV/AIDS severity
PEPFAR support has resulted in improved immune profiles for people living with HIV. One way of assessing the severity of the HIV burden is through CD4 lymphocyte counts, typically reported as the number of cells per cubic millimeter of blood (cells/mm³). In a healthy adult, the normal CD4 count ranges from about 500 to 1,600 cells/mm³. In HIV infection, the count gradually decreases as the disease progresses, which indicates a weakening immune system. AIDS is considered to be less than 200 cells/mm³. One analysis of Cameroon, Mozambique, Uganda, and Zimbabwe (all PEPFAR countries) showed that the percentage of HIV patients with test results indicating AIDS declined from 19.4% in 2012 to 16.1% in 2016.
The countries in this study have a higher HIV burden relative to other countries where PEPFAR operates, but these estimates give us perspective of how dire the situation is in countries where HIV is a significant burden. Crucially, without ART, people with AIDS typically survive about three years.
How easily HIV could mutate into no longer being effectively controlled with current treatments
HIV mutates very quickly. (This is a major reason there has not yet been a successful vaccine for the disease.) ART decreases the HIV virus’ ability to replicate within a person’s body. If people who previously received ART through PEPFAR were cut off from their medication, there is a chance that the medication would no longer work effectively if eventually resumed. There is a further chance that if these mutated forms spread, they may also be less easily suppressed by current medication.
Projecting the mortality impacts of PEPFAR cuts
In 2024, 20.6 million people were on ARTs through PEPFAR. If the PEPFAR waiver were to completely fail, how many people would we expect to die? According to the WHO, as of 2023, 86% of all people living with HIV knew their status, 77% were receiving ARTs, and 72% had suppressed viral loads. That means that roughly 6.5% of the population already on ARTs have detectable viral loads. This could be due to a variety of factors, including suboptimal adherence, drug resistance, or pharmacokinetic issues, such as malabsorption. Whatever the cause, incomplete suppression is strongly associated with higher mortality, and this is the group likely to be most at risk of death over the remainder of Trump’s term.
However, there is a lot of uncertainty here. If left untreated, the median time for HIV to progress to AIDS is between eight and 11 years. A person with untreated AIDS will live about three years. Somewhere between 10% and 20% of people are rapid progressors, developing AIDS within a few years after contracting HIV. But it is a challenge to know how quickly the entire population on ARTs might progress to AIDS if untreated. There is also the difficulty of estimating the risk of mortality for the population on ARTs. People who had initially progressed to AIDS before going on therapy reach the danger zone again sooner because they are starting from a lower CD4 baseline.
We can look to a few estimates as a baseline. Based on one trial, if adults whose CD4 counts were above 350 cells/mm³ were to pause ARTs — restarting only once their CD4 dropped below 250 — we would expect roughly two to three extra deaths for every 100 people within 16 months, or excess mortality of around 2%. Another study that looked at interruptions of ARTs found that excess mortality was 1.9%.
A reasonable median estimate for excess mortality over each year would be about 2% of a population. While the 25th and 75th percentile are inexact, we could estimate 1% for the 25th percentile and 3% for the 75th percentile to allow for quite a wide range of possibilities, as this is not a well-studied phenomenon (partly due to high coverage of ARTs), and both studies are from almost 20 years ago.
Thus, I forecast an interquartile range of [1% - 2% - 3%] of people cut off from ARTs dying each year. With 20.6 million people receiving ARTs through PEPFAR before the freeze, that would give us an interquartile range of [206,000 - 412,000 - 618,000] people dying after one year and [812,000 - 1,599,000 - 2,363,000] after four years.
Up to this point, I have looked only at the consequences of ending distribution of ARTs, and I have not included the other services PEPFAR provides. To understand the impact of PEPFAR’s other programs, we can look to its other spending directives. These have changed somewhat over time, but in general, 55% of funding is spent on treatment, 15% on palliative care, 20% on prevention, and 10% on orphans and vulnerable children (OVC).
The waiver focuses primarily on distribution of HIV medication, but how can we estimate the mortality impacts of these other programs that were not a part of the waiver? While the 15% on palliative care improves quality of life toward the end, it likely does not extend life significantly enough to affect our estimates. Prevention efforts will certainly have an impact over a longer time period, but in the short term, the loss of prevention funding isn’t likely to significantly impact mortality. I expect that the 10% saved for OVC does, however, have a notable impact on preventing deaths over four years, as infants and young children can die very quickly once they have HIV.
If we are to assume that the OVC funding is as effective as the funding for treatment, that would put us at ARTs accounting for 55/65 (about 85%) of lives saved. I think the actual percentage is lower, as prevention perhaps would have a minor impact over four years, but I think it is reasonable to assume that ARTs account for about 80% of lives saved every year through PEPFAR. We therefore must adjust our estimate by multiplying by 1.25, as my previous forecast, which looked only at ARTs, would underestimate the amount of lives saved. This gives us:
Deaths after one year: [257,500 - 515,000 - 772,500]
Deaths after four years: [1,015,000 - 1,998,750 - 2,953,750]
The biggest source of uncertainty here is to what extent PEPFAR, or what remains of it, resumes services. While PEPFAR secured a limited waiver to continue ART distribution on February 1, many implementing partners reported laying off staff when funding froze, and surveys on the ground suggest services have been heavily disrupted.
If services do resume, the number of deaths will most likely be lower than the estimates I have provided. However, the Trump administration’s decision to end most foreign aid was drastic, and I think it is important that the international community prepares for the contingency that, despite the waiver, PEPFAR’s ART assistance ceases entirely.
Jared Leibowich forecasts for multiple organizations, including Samotsvety, Swift Centre, Good Judgment, and Metaculus. He has won multiple forecasting competitions, including Good Judgment's In the News Competitions (2021, 2022) and The Economist’s The World Ahead Competition (2022). He can be reached at jleibowich@gmail.com.
Excellent analysis! It's always interesting to learn how other forecasters model such complex issues.
While the slowdown in the decline of new HIV cases coinciding with the start of PEPFAR is certainly due to multiple complex factors, it's plausible that the initiative's investment in scaling up testing and case identification played a significant role. The program likely found an important number of previously undiagnosed individuals, thus altering the perceived rate at which newly discovered cases were declining. The actual number of new infections might have been declining, while the measured rate stabilized.